Stanozolol, better known as Winstrol, is one of the most famous steroids of all time.
Many people who start a Winstrol cycle do so because they’ve heard it can help them build muscle, gain strength, and shed fat quickly—and for the most part, that’s true. Just take a look at some Winstrol before and after photos, and you’ll see impressive transformations.
Combine this with claims that Winstrol’s side effects are milder than many other steroids, and it’s easy to see why so many bodybuilders are eager to inject or ingest this powerful drug.
But while the “marketing” might be compelling, the reality is that Winstrol’s side effects are significant and outweigh the benefits for most people.
For instance, just a couple of cycles of Winstrol can lead to:
- Liver damage
- Heart disease
- Reduced natural testosterone and testicle size
- Achy joints
- Acne
- Toxin exposure
- And more
To learn more about these side effects, what Winstrol does, its benefits, and more, keep reading.
What Is Winstrol?
Winstrol, also known as “Winny,” is the brand name of a synthetic (man-made) anabolic steroid called stanozolol (stan-oh-zo-lol). It usually comes in two forms: Winstrol pills and as an injectable liquid referred to as “Winstrol Depot.”
Chemists developed Winstrol at Winthrop Laboratories 1962 by modifying a naturally occurring steroid called dihydrotestosterone (DHT) so that it produced stronger muscle-building effects with fewer masculinizing side effects.
In the 1960s, Winstrol was briefly approved for treating conditions like osteoporosis, muscle wasting, and growth insufficiency in children, but the FDA quickly banned it for all but a few rare medical conditions.
Winstrol is technically still approved for certain medical purposes, but no pharmaceutical companies in the United States have produced it since 2003.
While Winstrol is still available in Europe under the brand name Stromba, most of the Winstrol in the U.S. now comes from private labs “cooking” their own steroids in places like Mexico or Thailand.
What Does Winstrol Do?
The biggest benefit of Winstrol is its ability to help you pack on muscle rapidly.
But with so many anabolic steroids offering a similar benefit, what does Winstrol do that sets it apart?
To understand why so many athletes cycle Winstrol rather than other anabolic compounds, you need to understand how steroids work.
How Steroids Work
Most of your body’s cells have specialized proteins on their surfaces called androgen receptors.
Think of these receptors as mailboxes that only accept messages from testosterone and similar hormones circulating in your blood.
When a testosterone molecule or other steroid “attaches” to an androgen receptor, it delivers its message to the cell’s nucleus, giving instructions on how to behave.
Steroids typically tell cells to build muscle, something researchers refer to as a steroid’s anabolic effect.
However, they also send other signals called androgenic effects, which promote male characteristics, including body and facial hair growth, a deeper voice, a more pronounced jawline, aggression, and acne. These are usually the side effects steroid users want to avoid.
Researchers have known for decades that all steroids have both anabolic and androgenic effects. To quantify the balance between these effects, they developed the anabolic ratio, which compares a steroid’s muscle-building potential to its likelihood of causing unwanted side effects.
Testosterone is the baseline, and has an anabolic to androgenic ratio of 100:100.
Importantly, much of the research behind this ratio comes from studies on rat muscle—specifically the smooth muscle surrounding the anus. Since humans aren’t rats, and smooth muscle isn’t the same as skeletal muscle, we should take this ratio with a grain of salt.
Nevertheless, it’s still a useful starting point for estimating a steroid’s muscle-building potential versus its side effects.
Winstrol Benefits
Many bodybuilders and athletes love “Winny” because they believe its benefits outweigh its side effects.
However, Winstrol’s advantages aren’t always as clear-cut as they might seem.
Let’s break down the purported benefits of Winstrol and see how they stack up.
Less Masculinizing
One of Winstrol’s most touted benefits is that it boosts muscle growth more than testosterone while causing fewer androgenic side effects.
In practice, things aren’t quite this clear cut, though.
Winstrol‘s anabolic to androgenic ratio is 320:30, but due to the arcane laws of steroid science, this doesn’t mean a Winstrol cycle will build exactly three times more muscle than testosterone (more on why soon).
What it does mean is that, milligrams per milligram, Winstrol is more effective at building muscle than testosterone and produces fewer negative side effects.
This is particularly important when discussing Winstrol for women, who generally avoid highly androgenic drugs (like trenbolone) due to their harsh, masculinizing side effects.
For instance, when females take highly androgenic steroids, they can expect all the things men experience, including balding, increased body hair growth, acne, deepened voice, increased aggression, and infertility.
In addition, they may also experience:
- Clitoral enlargement (clitoromegaly)
- Masculine jawline growth
- Menstrual irregularities
- Breast shrinkage
- Birth defects
- Severe depression
Which is why many female bodybuilders who’ve taken powerful steroids for years end up looking and sounding like, well, men:
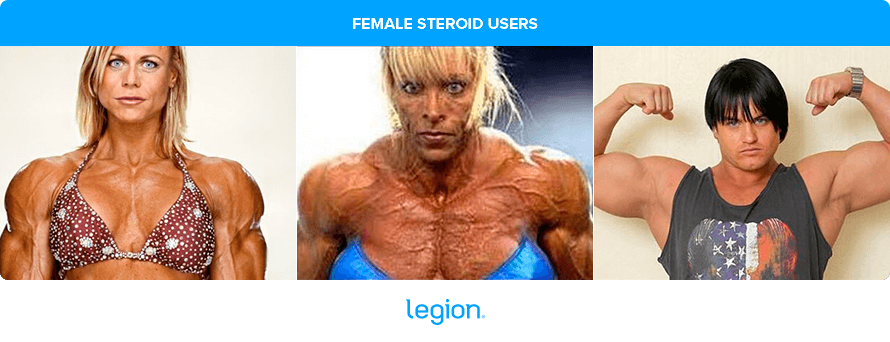
Thanks to its low androgenic score, Winstrol in women poses fewer risks, making it a popular choice for females who want the muscle-building benefits of steroids without turning into jacked gargoyles.
That said, there’s scant long-term research on how steroids affect women (or men), so it’s impossible to know what Winstrol side effects women would experience if they took it for years on end.
No Estrogen Conversion
Another benefit of Winstrol is that your body doesn’t convert it into estrogen, the primary female sex hormone. This is unlike most steroids, which typically raise estrogen levels.
In men, the enzyme aromatase converts a percentage of our testosterone into estrogen through a process called aromatization.
Normally, men maintain low estrogen levels. But when steroids skyrocket your testosterone levels, estrogen levels increase proportionally, leading to unwanted feminizing effects like gynecomastia (“man boobs”), water retention, and fat gain.
To counter these side effects, many athletes use estrogen blockers, but this approach has its own drawbacks.
Estrogen is crucial for muscle recovery, as it helps muscles absorb glucose, boosts anabolic hormone levels, and increases the number of androgen receptors in muscle cells. It also allows you to train harder by bolstering serotonin levels, which increases your arousal, focus, and ability to push yourself in workouts.
So, how is a roider to reap the benefits of estrogen without growing man boobs and getting bloated and fat?
Winstrol is part of the answer.
Because it doesn’t convert into estrogen, you can take it without worrying about these side effects. This is why Winstrol is the steroid of choice among many athletes looking to maximize muscle mass, strength, and performance, without the bloating and fat gain that often accompany other steroids.
However, there’s a trade-off.
Steroids that don’t increase estrogen levels are generally less effective for muscle growth. This is why people who only take a Winstrol cycle typically don’t make the dramatic size gains that people taking testosterone, Dianabol, and other estrogen-producing steroids do.
In other words, Winstrol’s muscle-building properties are hamstrung by its inability to raise estrogen levels, which is why it’s not as effective for building mass as pure testosterone, despite its higher anabolic score.
Thanks to its lack of aromatization into estrogen, Winstrol also produces little if any water retention or fat gain, which makes it an ideal steroid for cutting or lean bulking (or sprinting, if you’re Ben Johnson).
Enhances Other Steroids
Another reason many bodybuilders and athletes cycle Winstrol is that it works synergistically with other steroids to promote muscle growth.
It does this by reducing levels of sex-hormone binding globulin (SHBG) in the blood. SHBG is a protein that “blocks” the effects of testosterone by binding to it, preventing it from delivering its muscle-building signals to cells.
By reducing SHBG levels in the blood, Winstrol makes the other steroids you’re taking more potent, too.
Although all anabolic steroids reduce SHBG levels, Winstrol is particularly effective.
A good example of this comes from a study conducted by scientists at the University of Hamburg. The researchers had 25 young people take a stanozolol cycle (Winstrol) of 0.2 mg/kg per day for three days.
This is a typical Winstrol dosage for a small bodybuilder.
The scientists measured everyone’s SHBG and hormone levels before and for several days after they started taking Winstrol.
The results showed that Winstrol reduced SHBG levels by an average of 48% after just a week. In comparison, testosterone usually reduces SHBG levels by around 30%.
The takeaway is that Winstrol not only boosts its own muscle-building effects but also enhances the effectiveness of any other steroids you’re using. And that’s why most informed steroid users take a Winstrol cycle in addition to other steroids, like testosterone.
Winstrol Side Effects
Now that you know the “perks” of taking Winstrol, let’s look at its downsides.
The main warnings you find online are:
- Liver damage
- Heart disease
- Reduced natural testosterone levels and testicle size
- Achy joints
- Acne
- Toxin exposure
Sounds fun!
Let’s go over each.
Liver Damage
While stanozolol is available in both pill and injectable forms, most users prefer to take Winstrol pills.
Taking Winstrol pills is more convenient than injecting it—you don’t have to “pin” yourself several times weekly and pills are easier to conceal than needles and needle marks.
Taking steroids in pill form has significant drawbacks, though.
Injectable steroids bypass the liver and go directly into the bloodstream, allowing more of the compound to reach your muscles without stressing your liver.
In contrast, when you swallow most steroids, an enzyme in your liver called 17beta-hydroxysteroid dehydrogenase (17beta-HSD) breaks them down. Even if you took a whole bottle of testosterone pills, only a tiny fraction would enter your bloodstream—probably not enough to fail a drug test.
To prevent this from happening, chemists combine steroids with carbon and hydrogen atoms in a process called alkylation. This modification allows the steroids to pass through your liver intact and enter your bloodstream, where they quickly begin telling your muscles to grow.
The problem is that this process can damage your liver.
Scientists still aren’t sure exactly why or how this occurs, but the most plausible theory is that the liver is highly sensitive to anabolic steroids. When it isn’t able to break down the steroids—which is the case with oral steroids like stanozolol—the excess can cause liver damage and dysfunction.
The most common form of liver damage from Winstrol use is cholestasis, a condition where bile flow from the liver to the digestive system slows or stops.
This causes a buildup of bile salts, bilirubin, and other digestive compounds in the liver and blood, which leads to all kinds of problems including:
- Clay-colored stool
- Amber-colored urine
- Jaundice
- Itching
- Nausea
- Stomach pain
- Reduced appetite
- Fatigue
- Death of liver tissue
More severe symptoms can include liver inflammation, peliosis hepatis (blood-filled cysts on the liver), internal bleeding, and various forms of liver cancer.
Taking Winstrol pills doesn’t automatically result in liver damage, of course, and there may be things you can do to minimize your risk.
For instance, a 2018 study suggested exercise might offer some protection. It found that while Winstrol increases the risk of liver damage in rats, exercise helped reduce some of the harmful effects. It also found that the liver damage caused by Winstrol is “dose-dependent.”
In other words, Winstrol-induced liver damage probably only becomes an issue when you take high doses for long periods. This is why most informed steroid users limit Winstrol cycles to 8-to-12 weeks or less before giving their liver a break.
That said, the risks are still very real. Several case reports have detailed how otherwise healthy bodybuilders have died of liver cancer after taking oral steroids.
We also have no long-term studies investigating how different Winstrol dosages affect the liver.
Furthermore, we don’t fully understand how combining Winstrol, steroids of other varieties, and less potent anabolic compounds like SARMs might affect liver health. This leaves us with an incomplete picture of how a real-world steroid “stack” containing Winstrol affects the liver.
Thus, no matter how you slice it, Winstrol poses a serious risk to liver health.
Heart Disease
Winstrol can have serious effects on heart health, particularly on cholesterol levels.
It tends to lower HDL (good) cholesterol and raise LDL (bad) cholesterol, shifting the balance in a way that increases the risk of arteriosclerosis—a condition where arteries harden and narrow, leading to heart disease.
In one study published in the journal JAMA, healthy male weightlifters who took 6 mg of oral Winstrol daily for 6 weeks experienced a 33% drop in HDL cholesterol and a 29% increase in LDL cholesterol. Together, these changes put them at greater risk of cardiovascular disease.
Even injectable Winstrol isn’t safe for the heart. In a study of 12 healthy men, a single 50-mg Winstrol injection led to a 30% drop in HDL cholesterol and a 33% increase in LDL cholesterol. Worryingly, these changes remained elevated for four weeks.
Reduced Natural Testosterone Levels and Testicle Size
Like every other steroid, Winstrol reduces your natural testosterone levels. This is an unavoidable, intractable, inherent side effect of all steroids—you can’t reduce, modify, or change it whatsoever.
To understand why, let’s look at how your body produces testosterone:
- Your testes (or ovaries in women) produce testosterone. If your “T” levels dip, a portion of the brain called the hypothalamus senses the decrease and releases a hormone called Gonadotropin-Releasing Hormone (GnRH).
- The pituitary gland detects the increased GnRH levels and produces luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which trigger specialized cells in the testes known as Leydig cells to produce testosterone.
- As testosterone levels rise, the hypothalamus produces less GnRH, testosterone production decreases, and the cycle repeats itself.
Assuming someone is otherwise healthy, this system does a remarkably good job of keeping testosterone levels within a relatively narrow range.
Everything changes when you introduce anabolic steroids, though.
The sudden surge in testosterone causes the hypothalamus to drastically reduce GnRH production, which shuts down LH and FSH production and halts natural testosterone production.
Within days of taking steroids, natural testosterone levels plummet, and over several months, your testicles shrink.
In the case of Winstrol, the suppressive effect on testosterone is sizable. For instance, in a study published in Clinical Endocrinology, men given 10 mg of Winstrol daily for 2 weeks saw their testosterone levels fall by 55%.
The only way to restore natural testosterone production and testicle size is to stop taking steroids. Even then, it can take several months before testosterone levels and testicle size return to normal.
Achy Joints
An internet search for Winstrol’s side effects will often bring up claims that it makes joints feel achy, sore, and stiff. These claims are likely misguided.
Winstrol causes little to no water retention, which makes you look leaner, “fuller,” and “drier.” Bodybuilders often mistakenly make the apocryphal claim that Winstrol does this by “pulling water out of your joints.”
They’re wrong.
While Winstrol doesn’t cause significant water retention like other steroids, it doesn’t dehydrate you or pull water from your joints (or any other part of your body).
There are two more likely reasons why bodybuilders complain of joint pain when taking Winstrol:
- They read it online, expected it to happen, and then experienced joint pain thanks to the nocebo effect.
- They were training harder, more often, and with more volume (sets)—common benefits of Winstrol use. The increased training volume and intensity likely caused the joint soreness, not the Winstrol itself.
In reality, steroids generally promote tissue growth, healing, and recovery, so you’d expect steroids (Winstrol included) to make your joints more durable, resilient, and strong while you’re taking them—not weaker.
Acne
Acne is caused by bacteria residing in the skin’s oil. Scientists aren’t entirely sure why or how it flares up, but anything that increases oil production in the skin—like the surge in androgenic hormones in adolescence—tends to trigger it.
Steroids like testosterone also boost the skin’s oil production, which can lead to breakouts or make existing acne worse.
Typically, the acne that accompanies steroid use is most severe around the shoulders, chest, and upper back, like this:
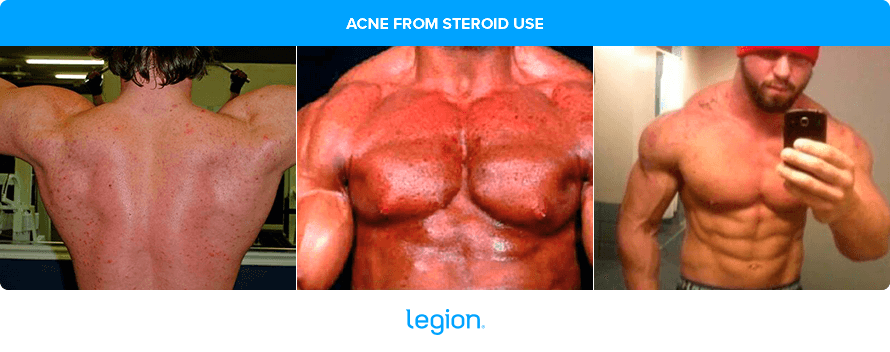
And if you’re thinking you’re safe because you don’t have acne now, think again.
Pete Rubish, a powerlifter who’s been open about his steroid use, also had clear skin before he started taking steroids. After a few months of taking steroids he says, “It’s so bad that if someone literally just pats you on the back you’re in horrible pain.”
More disturbingly, he said it also got worse after he stopped taking drugs, and it didn’t go away until he went to a dermatologist and started taking acne medication.
There isn’t much direct research on Winstrol and acne, but it appears to be milder than testosterone in this regard.
That said, everyone’s reaction to Winstrol varies, and it’s possible some people might get more or less acne than others.
Although acne is a temporary side effect of Winstrol use, it can cause permanent scarring.
Toxin Exposure
No companies currently produce Winstrol for human use, so when you buy it, you’re putting your health and life in the hands of private labs or individuals who obtain it from pharmaceutical companies making Winstrol for animals.
These products undergo no formal oversight, regulation, or testing, which means the product you end up with could be counterfeit, tainted, and watered-down.
Tainted steroids are particularly dangerous because they can contain toxins like heavy metals, pathogens, and various contaminants, which may cause a long list of health problems that may not show up until years after you’ve stopped taking steroids.
We don’t know what percentage of steroids on the market are tainted, but it’s likely significant. For example, a study conducted by the Center for Preventative Doping Research found that 34% of 70 anabolic steroids seized in police raids didn’t contain the ingredients listed on the label.
They also found that without sophisticated testing methods, it’s often difficult to tell real steroids from fakes.
Unlike some other drugs, there are no reliable at-home tests to check the purity of steroids. All steroid users can do is try to find a trusted supplier, inspect the packaging as carefully as possible, and hope for the best.
Other Side Effects
Here’s a short list of the some of the less severe side effects associated with taking a Winstrol cycle:
- Insomnia
- Night sweats
- Increased blood pressure
- Hair loss
- Erectile dysfunction
- Infertility
- Increased aggression
- Increased risk of prostate, brain, and breast cancer
- Permanent testicular atrophy
- Insulin resistance
- Nosebleeds
FAQ #1: How can you tell if someone is on Winstrol?
Winstrol results aren’t as striking as the results you get from other anabolic steroids, so it can be surprisingly difficult to tell if someone is “natty or not” if they’re only taking a Winstrol cycle.
For example, here’s a good example of some Winstrol before and after photos of someone who is relatively new to weightlifting after an 8-week Winstrol cycle:

While the guy obviously made much faster progress than you could achieve naturally, it’s not obvious he’s “on steroids.”
Here are five more examples of athletes who were caught taking Winstrol:

All of them look fit and muscular, but none scream “enhanced athlete.”
The point is this: Not everyone takes steroids to get jacked. Steroids also enhance sports performance and recovery. For many, muscle gain is just a side effect, not the primary goal.
Unless someone is an IFBB pro or looks like one, it’s rarely obvious if someone is on steroids at all, much less what they’re taking. The only way to know for sure is to take repeated blood tests over a long period when they’re looking and performing their best, and that simply isn’t feasible.
Barring that, you can estimate the chances someone’s on steroids by looking at their fat-free mass index (FFMI), a measurement of how much muscle they have per unit of height. When someone’s FFMI is above a certain threshold, the odds they’re on steroids skyrocket.
If you want to calculate someone’s FFMI and learn more about this measurement tool, check out the Legion FFMI Calculator.
FFMI will only tell you whether or not someone’s taking steroids, though—it can’t confirm what someone is taking.
FAQ #2: Winstrol vs. Anavar: What’s the difference?
Anavar, also known as oxandrolone, is an anabolic steroid chemically altered to produce fewer androgenic (masculinizing) side effects. This makes it a favorite among female bodybuilders, physique competitors, and Instagram fitness personalities.
Many people compare Winstrol vs. Anavar because they tend to have milder side effects than traditional steroids and they’re taken orally in pill form. Although some steroid-users claim that Anavar produces fewer side effects than Winstrol, no scientific studies have compared the effects of these two drugs.
FAQ #3: Is Winstrol legal?
No.
It is illegal to use anabolic steroids like Winstrol in most countries without a prescription. In the United States, anabolic steroids like Winstrol are Schedule III controlled substances, which means taking them comes with big fines and potential jail time.
Winstrol is also banned by most sports federations including the United States Anti-Doping Administration (USADA), the World Anti-Doping Administration (WADA), and the International Olympic Committee (IOC).
FAQ #4: Does Winstrol burn fat?
No, Winstrol doesn’t directly burn fat. However, people often link Winstrol and fat loss.
This connection likely arises because Winstrol doesn’t convert to estrogen in the body, so it doesn’t cause water retention like other steroids. As a result, your muscles appear “denser” and less “puffy” when taking Winstrol, which creates the illusion that it burns fat.
Adding to this misconception is the fact that bodybuilders often use Winstrol during cutting cycles. Since it allows them to continue building muscle without water obscuring their results, people often assume physique competitors use Winstrol for fat loss during these phases. This, however, is a misunderstanding.
Winstrol is also popular among athletes in sports where staying lean is essential, which likely reinforces the association between Winstrol and fat loss. These athletes choose Winstrol because it promotes muscle growth without adding bulk to their body in the form of water, which helps them maintain peak performance.
Scientific References +
- Davey, Rachel A, and Mathis Grossmann. “Androgen Receptor Structure, Function and Biology: From Bench to Bedside.” The Clinical Biochemist. Reviews, vol. 37, no. 1, Feb. 2016, pp. 3–15, www.ncbi.nlm.nih.gov/pmc/articles/PMC4810760/.
- Kicman, A T. “Pharmacology of Anabolic Steroids.” British Journal of Pharmacology, vol. 154, no. 3, June 2008, pp. 502–521, www.ncbi.nlm.nih.gov/pmc/articles/PMC2439524/, https://doi.org/10.1038/bjp.2008.165.
- FALLIERS, CONSTANTINE J. “Anabolic Effects of Stanozolol.” American Journal of Diseases of Children, vol. 106, no. 4, 1 Oct. 1963, p. 388, https://doi.org/10.1001/archpedi.1963.02080050390008. Accessed 20 Apr. 2022.
- Ramasamy, Ranjith, et al. “The Role of Estradiol in Male Reproductive Function.” Asian Journal of Andrology, vol. 18, no. 3, 2016, p. 435, www.ncbi.nlm.nih.gov/pmc/articles/PMC4854098/, https://doi.org/10.4103/1008-682x.173932.
- KNUDSEN, JAMES F., and STEPHEN R. MAX. “Aromatization of Androgens to Estrogens Mediates Increased Activity of Glucose 6-Phosphate Dehydrogenase in Rat Levator Ani Muscle*.” Endocrinology, vol. 106, no. 2, Feb. 1980, pp. 440–443, https://doi.org/10.1210/endo-106-2-440. Accessed 7 Dec. 2021.
- Hobbs, Curtis, et al. “Testosterone Administration Increases Insulin-like Growth Factor-I Levels in Normal Men.” The Journal of Clinical Endocrinology & Metabolism, vol. 77, no. 3, 1 Sept. 1993, pp. 776–779, https://doi.org/10.1210/jcem.77.3.7690364. Accessed 20 Nov. 2023.
- Ho, Ken K.Y., et al. “Sex Steroid Regulation of Growth Hormone Secretion and Action.” Hormone Research, vol. 45, no. 1-2, 1996, pp. 67–73, https://doi.org/10.1159/000184762. Accessed 2 Feb. 2021.
- Weissberger, A. J., and K. K. Ho. “Activation of the Somatotropic Axis by Testosterone in Adult Males: Evidence for the Role of Aromatization.” The Journal of Clinical Endocrinology and Metabolism, vol. 76, no. 6, 1 June 1993, pp. 1407–1412, pubmed.ncbi.nlm.nih.gov/8501143/, https://doi.org/10.1210/jcem.76.6.8501143.
- Rance, Naomi E, and Stephen R Max. “Modulation of the Cytosolic Androgen Receptor in Striated Muscle by Sex Steroids*.” Endocrinology, 1 Jan. 1984, https://doi.org/10.1210/endo-115-3-862.
- Dickerson, Lori M., et al. “Premenstrual Syndrome.” American Family Physician, vol. 67, no. 8, 15 Apr. 2003, pp. 1743–1752, pubmed.ncbi.nlm.nih.gov/12725453/.
- Selby, C. “Sex Hormone Binding Globulin: Origin, Function and Clinical Significance.” Annals of Clinical Biochemistry, vol. 27 ( Pt 6), 1990, pp. 532–41, www.ncbi.nlm.nih.gov/pubmed/2080856, https://doi.org/10.1177/000456329002700603.
- GERNOT SINNECKER, and SIGRUN KÖHLER. “Sex Hormone-Binding Globulin Response to the Anabolic Steroid Stanozolol: Evidence for Its Suitability as a Biological Androgen Sensitivity Test*.” The Journal of Clinical Endocrinology & Metabolism, vol. 68, no. 6, 1 June 1989, pp. 1195–1200, pubmed.ncbi.nlm.nih.gov/2723028/, https://doi.org/10.1210/jcem-68-6-1195. Accessed 22 Aug. 2024.
- Plymate, Stephen R, et al. “Sex Hormone-Binding Globulin Changes with Androgen Replacement.” The Journal of Clinical Endocrinology and Metabolism, vol. 57, no. 3, 1 Sept. 1983, pp. 645–648, https://doi.org/10.1210/jcem-57-3-645. Accessed 27 Apr. 2023.
- Labrie, Fernand, et al. “The Key Role of 17β-Hydroxysteroid Dehydrogenases in Sex Steroid Biology.” Steroids, vol. 62, no. 1, Jan. 1997, pp. 148–158, https://doi.org/10.1016/s0039-128x(96)00174-2. Accessed 28 Feb. 2021.
- Hinchliffe, S A, et al. “Cellular Distribution of Androgen Receptors in the Liver.” Journal of Clinical Pathology, vol. 49, no. 5, 1 May 1996, pp. 418–420, www.ncbi.nlm.nih.gov/pmc/articles/PMC500485/.
- Krüskemper, Hans L., and Georg Noell. “Liver Toxicity of a New Anabolic Agent: Methyltrienolone (17α-Methyl-4,9,11-Estratriene-17β-Ol-3-One).” Steroids, vol. 8, no. 1, July 1966, pp. 13–24, https://doi.org/10.1016/0039-128x(66)90114-0. Accessed 18 Sept. 2021.
- Sánchez-Osorio, Magdalena, et al. “Anabolic-Androgenic Steroids and Liver Injury.” Liver International, vol. 28, no. 2, 27 Sept. 2007, pp. 278–282, https://doi.org/10.1111/j.1478-3231.2007.01579.x.
- Nguyen, Ken D, et al. “Atypical Causes of Cholestasis.” World Journal of Gastroenterology : WJG, vol. 20, no. 28, 28 July 2014, pp. 9418–9426, www.ncbi.nlm.nih.gov/pmc/articles/PMC4110573/, https://doi.org/10.3748/wjg.v20.i28.9418.
- Štimac, Davor, et al. “Androgenic/Anabolic Steroid-Induced Toxic Hepatitis.” Journal of Clinical Gastroenterology, vol. 35, no. 4, Oct. 2002, pp. 350–352, https://doi.org/10.1097/00004836-200210000-00013. Accessed 11 May 2020.
- Cabasso A. “Peliosis Hepatis in a Young Adult Bodybuilder.” Medicine and Science in Sports and Exercise, vol. 26, no. 1, 2022, pubmed.ncbi.nlm.nih.gov/8133732/. Accessed 22 Aug. 2024.
- Winwood, P. J., et al. “Bleeding Oesophageal Varices Associated with Anabolic Steroid Use in an Athlete.” Postgraduate Medical Journal, vol. 66, no. 780, 1 Oct. 1990, pp. 864–865, https://doi.org/10.1136/pgmj.66.780.864. Accessed 12 Nov. 2019.
- Hernandez-Nieto L;Bruguera M;Bombi J;Camacho L;Rozman C. “Benign Liver-Cell Adenoma Associated with Long-Term Administration of an Androgenic-Anabolic Steroid (Methandienone).” Cancer, vol. 40, no. 4, 2015, pubmed.ncbi.nlm.nih.gov/198105/, https://doi.org/10.1002/1097-0142(197710)40:4%3C1761::aid-cncr2820400454%3E3.0.co;2-c. Accessed 22 Aug. 2024.
- Evert, M, and F Dombrowski. “Hepatozelluläre Karzinome in Der Nichtzirrhotischen Leber.” Der Pathologe, vol. 29, no. 1, 6 Dec. 2007, pp. 47–52, pubmed.ncbi.nlm.nih.gov/18057936/, https://doi.org/10.1007/s00292-007-0953-3. Accessed 22 Aug. 2024.
- Ozcagli, Eren, et al. “Stanozolol Administration Combined with Exercise Leads to Decreased Telomerase Activity Possibly Associated with Liver Aging.” International Journal of Molecular Medicine, vol. 42, no. 1, 1 July 2018, pp. 405–413, www.ncbi.nlm.nih.gov/pmc/articles/PMC5979936/, https://doi.org/10.3892/ijmm.2018.3644.
- Gorayski, P, et al. “Hepatocellular Carcinoma Associated with Recreational Anabolic Steroid Use.” British Journal of Sports Medicine, vol. 42, no. 1, 5 June 2007, pp. 74–75, https://doi.org/10.1136/bjsm.2007.03932. Accessed 22 Mar. 2021.
- Hardt, Aline, et al. “Development of Hepatocellular Carcinoma Associated with Anabolic Androgenic Steroid Abuse in a Young Bodybuilder: A Case Report.” Case Reports in Pathology, vol. 2012, 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3420693/, https://doi.org/10.1155/2012/195607. Accessed 11 May 2020.
- Thompson, P. D., et al. “Contrasting Effects of Testosterone and Stanozolol on Serum Lipoprotein Levels.” JAMA, vol. 261, no. 8, 24 Feb. 1989, pp. 1165–1168, pubmed.ncbi.nlm.nih.gov/2915439/. Accessed 18 Feb. 2023.
- Small, M, et al. “The Effect of Intramuscular Stanozolol on Fibrinolysis and Blood Lipids.” Thrombosis Research, vol. 28, no. 1, 1 Oct. 1982, pp. 27–36, pubmed.ncbi.nlm.nih.gov/6891506/, https://doi.org/10.1016/0049-3848(82)90030-5. Accessed 22 Aug. 2024.
- Burger, Henry G. “Androgen Production in Women.” Fertility and Sterility, vol. 77, 1 Apr. 2002, pp. 3–5, www.fertstert.org/article/S0015-0282(02)02985-0/fulltext, https://doi.org/10.1016/S0015-0282(02)02985-0.
- Tyagi, Vineet, et al. “Revisiting the Role of Testosterone: Are We Missing Something?” Reviews in Urology, vol. 19, no. 1, 2017, pp. 16–24, www.ncbi.nlm.nih.gov/pmc/articles/PMC5434832/, https://doi.org/10.3909/riu0716. Accessed 12 May 2020.
- Rosenfield, R L, et al. “Acute Hormonal Responses to the Gonadotropin Releasing Hormone Agonist Leuprolide: Dose-Response Studies and Comparison to Nafarelin–a Clinical Research Center Study.” The Journal of Clinical Endocrinology & Metabolism, vol. 81, no. 9, Sept. 1996, pp. 3408–3411, https://doi.org/10.1210/jcem.81.9.8784105. Accessed 31 Mar. 2023.
- Nedresky, Daniel, and Gurdeep Singh. “Physiology, Luteinizing Hormone.” PubMed, StatPearls Publishing, 2020, www.ncbi.nlm.nih.gov/books/NBK539692/.
- Kerr, James B, and Richard M Sharpe. Follicle-Stimulating Hormone Induction of Ley Dig Cell Maturation. Vol. 116, no. 6, 1 June 1985, pp. 2592–2604, https://doi.org/10.1210/endo-116-6-2592. Accessed 31 May 2023.
- Hoffman, Jay R, and Nicholas A Ratamess. “Medical Issues Associated with Anabolic Steroid Use: Are They Exaggerated?” Journal of Sports Science & Medicine, vol. 5, no. 2, 2006, pp. 182–93, www.ncbi.nlm.nih.gov/pmc/articles/PMC3827559/.
- SMALL, M, et al. “ALTERATION of HORMONE LEVELS in NORMAL MALES given the ANABOLIC STEROID STANOZOLOL.” Clinical Endocrinology, vol. 21, no. 1, 1 July 1984, pp. 49–55, pubmed.ncbi.nlm.nih.gov/6430603/, https://doi.org/10.1111/j.1365-2265.1984.tb00135.x. Accessed 22 Aug. 2024.
- Lynn, Darren, et al. “The Epidemiology of Acne Vulgaris in Late Adolescence.” Adolescent Health, Medicine and Therapeutics, vol. 7, Jan. 2016, p. 13, www.ncbi.nlm.nih.gov/pmc/articles/PMC4769025/, https://doi.org/10.2147/ahmt.s55832.
- Király, C. L., et al. “Effect of Testosterone and Anabolic Steroids on the Size of Sebaceous Glands in Power Athletes.” The American Journal of Dermatopathology, vol. 9, no. 6, 1 Dec. 1987, pp. 515–519, pubmed.ncbi.nlm.nih.gov/3445928/, https://doi.org/10.1097/00000372-198712000-00008. Accessed 16 Sept. 2021.
- da Justa Neves, Diana Brito, et al. “Incidence of Anabolic Steroid Counterfeiting in Brazil.” Forensic Science International, vol. 228, no. 1-3, May 2013, pp. e81–e83, https://doi.org/10.1016/j.forsciint.2013.02.035. Accessed 27 Aug. 2021.
- Abbate, V., et al. “Anabolic Steroids Detected in Bodybuilding Dietary Supplements – a Significant Risk to Public Health.” Drug Testing and Analysis, vol. 7, no. 7, 6 Oct. 2014, pp. 609–618, https://doi.org/10.1002/dta.1728.
- Neves, Diana Brito da Justa, and Eloisa Dutra Caldas. “GC–MS Quantitative Analysis of Black Market Pharmaceutical Products Containing Anabolic Androgenic Steroids Seized by the Brazilian Federal Police.” Forensic Science International, vol. 275, June 2017, pp. 272–281, www.toxicologia.unb.br/admin/ckeditor/kcfinder/upload/files/2017%20FSI.pdf, https://doi.org/10.1016/j.forsciint.2017.03.016. Accessed 5 Sept. 2021.
- Câmara, Lucas Caseri . Anabolic Androgenic Steroids from Underground Market: Drug Quality and Implications for Research. July 2023, pp. 12(3):59-64, www.researchgate.net/publication/372647253_Anabolic_Androgenic_Steroids_from_Underground_Market_drug_Quality_and_Implications_for_Research, http://dx.doi.org/10.9734/AJRIMPS/2023/v12i3221.
- Thevis, Mario , et al. Analysis of Confiscated Black Market Drugs Using Chromatographic and Mass Spectrometric Approaches. Apr. 2008.